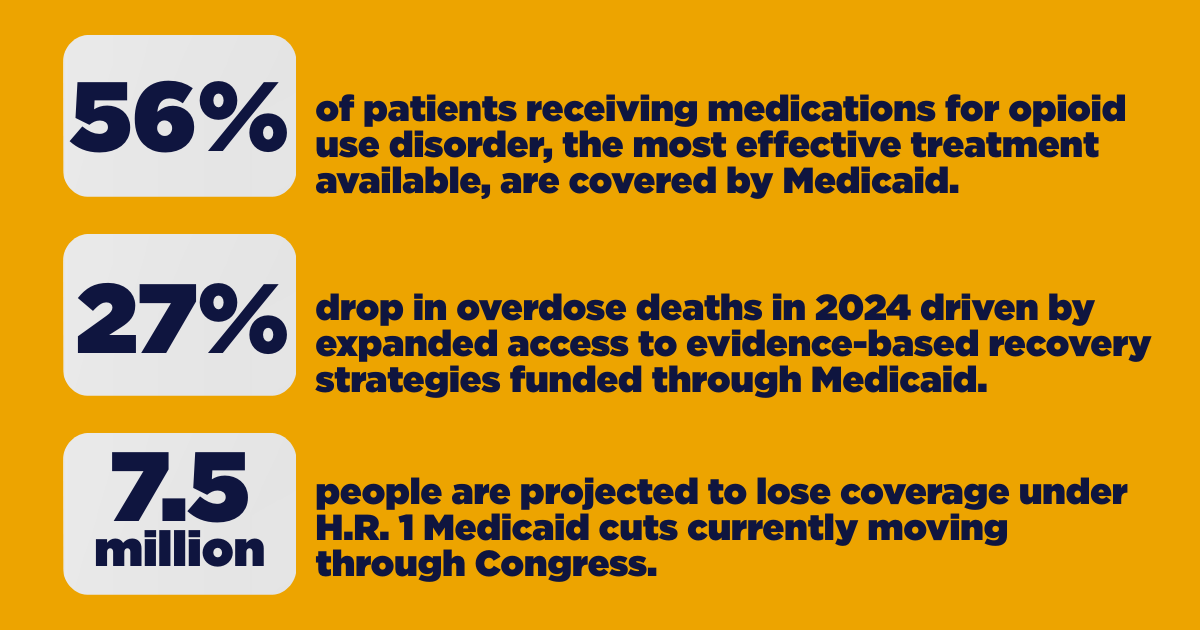
Overdose deaths fell 27%, the largest single-year drop in decades. That happened because people could get to treatment, stay on their medications, and access the wrap-around support that keeps someone alive, at home, and in their community. Medicaid made most of that possible. That progress is now directly at risk.
Not because the evidence against these services is clear, but because fraud investigations and blanket funding freezes are being treated as the same thing and they are not.
What is Happening
In January 2026, CMS deferred hundreds of millions in Medicaid funding in Minnesota, targeting peer support specialists, non-emergency medical transportation and housing stabilization services. Investigations have since expanded to California, Maine, and New York. Congressional oversight committees have sent letters to ten states demanding documentation, with days, not weeks, to respond.
Here is the core problem: fraud investigations and blanket funding freezes are not the same thing. The first targets bad actors. The second cuts off everyone, including the patients currently in or seeking care. That distinction matters enormously.
It is also not clear what states are actually supposed to do. The demands are broad. The timelines are punishing. There is no defined process for demonstrating compliance or getting funding restored. States are being asked to fix something without being told what fixing it looks like.
There is no defined process for demonstrating compliance or getting funding restored. Without one, states cannot fix the problem and patients cannot wait while they figure it out.
There is no defined process for demonstrating compliance or getting funding restored. Without one, states cannot fix the problem and patients cannot wait while they figure it out.
What is at Stake
The services under investigation are not redundant line items. They are the infrastructure that determines whether any other treatment can work at all.
Peer support and recovery specialists are certified professionals who draw on their own experience of addiction to keep patients engaged in treatment. Research shows that relationship cuts emergency department visits, reduces hospitalizations and lowers costs. It is a clinical intervention and not a social nicety.
Non-emergency medical transportation is the only thing standing between many patients and a missed appointment. License suspensions and the absence of rural transit are real obstacles. For someone without transit, a missed appointment is not just a scheduling problem. It is a treatment failure.
Housing stabilization is part of the clinical picture too. For someone in recovery, unstable housing is a medical risk factor. Treating it as a peripheral social service misunderstands what recovery actually requires.
Defunding these services does not target fraud. It dismantles the infrastructure recovery depends on.
Accountability Has a Target
We support Medicaid oversight that is precise, evidence-based and conducted with due process. Real oversight involves specific findings, clear legal process and collaboration with states on a defined path to resolution. The actions taken in Minnesota, California, Maine and New York have raised serious questions about whether that standard is being met.
When wrongdoing occurs, it should be addressed, swiftly and fully. But accountability must be precise. There is a meaningful difference between investigating specific bad actors and freezing funding for an entire category of services before the evidence is assembled. Spending more on behavioral health is not, by itself, evidence of fraud. Treating it that way has consequences for real people.
Funding disruptions do not reduce the problem. They relocate it, into emergency rooms and crisis centers, at higher cost, with no pathway to sustained recovery. Freezing access to care for the people who depend on these services, before specific wrongdoing has been demonstrated, is not a measured response. It is a policy choice with real consequences for real people.
Our Position
The 2024 overdose data proved what the evidence has long supported: lives are saved when people have consistent access to evidence-based recovery support. Peer support, transportation, stable housing — these are not peripheral. The difference between someone staying in recovery and someone dying.
Congress helped build that infrastructure. Legitimate oversight should protect it, not dismantle it, through broad freezes, impossible timelines and no clear path forward for the states and patients caught in the middle.